Most people think carpal tunnel syndrome is just a bad wrist ache. But it’s not. It’s a nerve being crushed-slowly, silently-until your hand stops working the way it should. If you’ve woken up with numb fingers, or dropped things you used to grip easily, you’re not imagining it. You’re experiencing carpal tunnel syndrome, the most common nerve compression problem in the upper body. And if you ignore it, it won’t go away. It’ll get worse.
What’s Really Happening Inside Your Wrist?
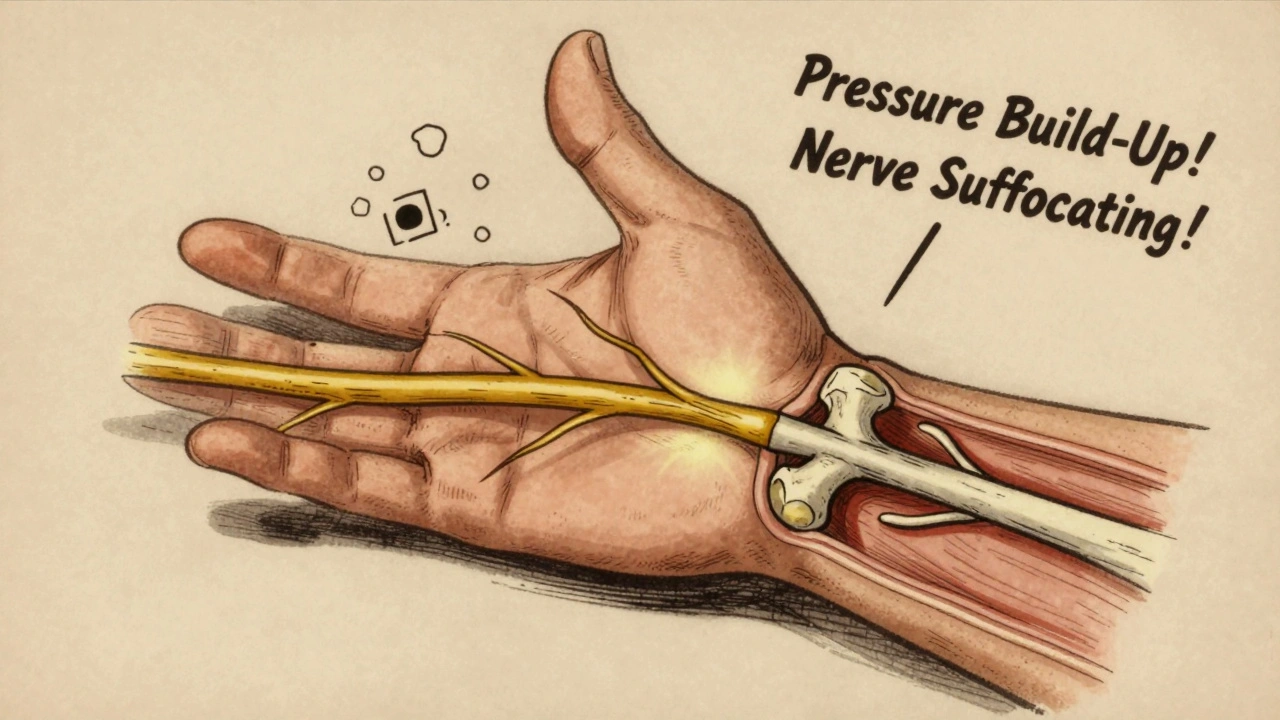
Your wrist isn’t just bone and skin. It’s a tight tunnel made of bones on the bottom and a tough ligament on top. Inside that tunnel, nine tendons bend your fingers, and one critical nerve-the median nerve-runs through, sending signals to your thumb, index, middle, and half your ring finger. When that tunnel gets crowded, the nerve gets squeezed. No room to breathe. No space to send signals. That’s when numbness, tingling, and burning start. It doesn’t happen overnight. Early on, symptoms creep in at night. You wake up shaking your hand like you’re trying to甩掉水珠. That’s your body’s desperate attempt to reset the nerve. But if you keep typing, gripping tools, or scrolling on your phone for hours, the pressure builds. The nerve’s blood flow slows. Swelling grows. And over time, the nerve’s outer coating starts to peel away. That’s when numbness turns permanent. Muscle weakness follows. Then you can’t button your shirt. Can’t open a jar. Can’t hold a coffee cup without dropping it.How Do You Know It’s Carpal Tunnel?
There’s no single test. Doctors use a mix of clues. The classic signs? Numbness in the thumb side of your hand, especially at night. Pain that travels up your forearm. Tingling when you hold your phone or drive. If you press on the center of your wrist and feel a shock shooting into your fingers-that’s the Tinel sign. If you bend your wrist forward for a minute and symptoms flare-that’s the Phalen test. These aren’t fancy tricks. They’re simple, reliable checks used in clinics from Manchester to Memphis. For confirmation, doctors may order nerve conduction studies. These measure how fast signals travel through the median nerve. If it’s slower than 3.7 milliseconds across the wrist, that’s a red flag. But here’s the catch: some people over 60 have abnormal test results but no symptoms. That’s why doctors don’t rely on tests alone. They look at your whole story-what you do all day, how long symptoms have lasted, whether your thumb muscles are shrinking. Then they decide.Conservative Treatments That Actually Work
If you catch it early-before the nerve is permanently damaged-conservative care works in 60 to 70% of cases. The #1 recommendation? A wrist splint worn at night. Not just any splint. One that holds your wrist straight, not bent. Wearing it for 6-8 hours every night for 4-6 weeks gives the nerve space to calm down. Many people report 60-80% improvement. It’s not glamorous. But it’s cheap. And it works. Add in nerve gliding exercises. These aren’t stretches you find on YouTube. They’re specific movements designed to help the median nerve slide smoothly through the tunnel. A physical therapist shows you how to do them-usually in 2-4 sessions. Then you do them daily. Combine that with avoiding positions that bend your wrist past 30 degrees-like cradling your phone or typing with your wrists dropped-and you’re already ahead of most people. Corticosteroid injections? They help too. About 70% of patients get relief for 3-6 months. It’s not a cure. But it buys time. Especially if you’re waiting to see a specialist, or you need to get through a busy season at work. The downside? Repeated injections can weaken tendons. So most doctors limit them to two or three over a year.When Surgery Becomes Necessary
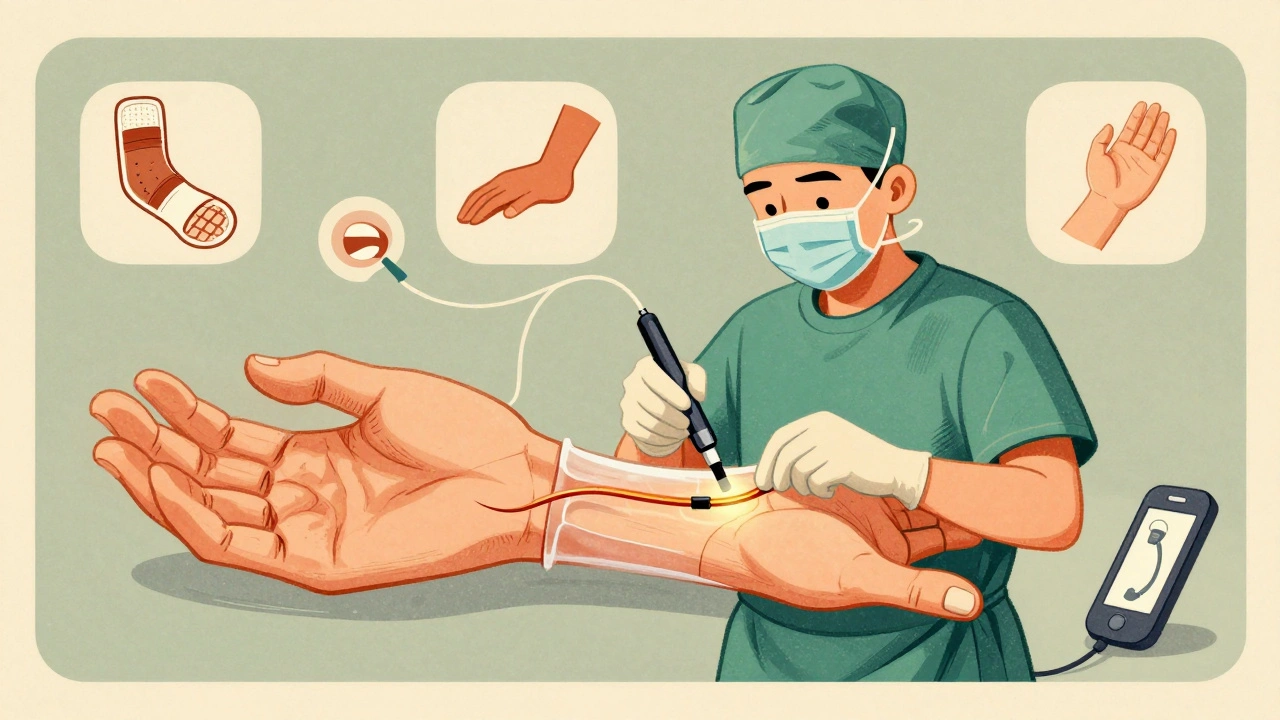
If you’ve tried splints, exercises, and injections for 6-8 weeks and you’re still losing sensation or strength-especially if your thumb muscles are shrinking-you need surgery. Not because you failed. Because the nerve is running out of time. There are two main options: open release and endoscopic release. Open release means a small cut along your palm, cutting the ligament to open the tunnel. Endoscopic uses a tiny camera through one or two smaller cuts. Both have the same success rate: 90-95%. But endoscopic often means less pain and faster recovery-about 2-3 weeks quicker. The new kid on the block? Ultrasound-guided percutaneous release. Approved by the FDA in 2021, this technique uses a tiny knife guided by real-time ultrasound. No big incision. Less pain. Patients return to work 50% faster. It’s not everywhere yet, but it’s growing fast. Post-surgery, you’ll need physical therapy-usually 6-8 sessions over 4-6 weeks. Most people go back to light work in 2-3 weeks. But if you’re a construction worker, a nurse, or a chef? You’ll need 10-12 weeks before you’re back to heavy lifting or repetitive motion.
What Doesn’t Work (And Why People Waste Money)
You’ll see ads for magnetic wristbands, copper bracelets, or “nerve detox” supplements. None of them have scientific backing. The same goes for acupuncture-some people swear by it, but studies show no real benefit over placebo. And don’t expect painkillers to fix this. Ibuprofen might dull the ache, but it won’t reduce the pressure on the nerve. That’s like putting a bandage on a broken pipe. Also, don’t wait for “the pain to get worse” before acting. The longer you delay, the less likely conservative care will work. Studies show people with symptoms under 10 months have a 75% chance of avoiding surgery. After 12 months? That drops to 35%.Who’s Most at Risk?
It’s not just office workers. Women over 45 are three times more likely to get it than men. Why? Smaller carpal tunnels. Hormones. Pregnancy can trigger it. So can diabetes, thyroid issues, or arthritis. But your job matters too. Assembly line workers, healthcare staff, meatpackers, and cashiers have the highest rates. Why? Repetitive motion. Forceful gripping. Prolonged wrist flexion. The Bureau of Labor Statistics recorded over 27,000 work-related CTS cases in 2022. Manufacturing, healthcare, and food service lead the list. Even if you’re not in a “high-risk” job, your phone habits might be. Scrolling for hours with your wrist bent? That’s a slow burn. The average person spends 3-5 hours a day on their phone. That’s 1,000+ hours a year with your wrist in a compressed position.What You Can Do Today
Don’t wait for the numbness to spread. Don’t assume it’ll go away. Here’s what to do now:- Buy a wrist splint (look for one that holds your wrist at 0-10 degrees extension). Wear it every night.
- Stop bending your wrist. Adjust your keyboard height. Use a stand for your phone. Keep your wrists neutral.
- Do 5 minutes of median nerve glides daily. Google “CTS nerve glide exercise” and follow a video from a physical therapist.
- See a doctor if symptoms last more than two weeks. Don’t self-diagnose. Other conditions mimic CTS.
- If you’re in a high-repetition job, talk to your employer about ergonomic adjustments. You have rights.
What Happens If You Do Nothing?
The nerve doesn’t heal itself. It degenerates. First, you lose feeling. Then, your thumb muscles waste away. That’s permanent. No surgery can bring back dead nerve tissue. You’ll lose grip strength. Fine motor skills. The ability to feel heat, cold, or pain in your fingers. That’s not just inconvenient. It’s life-changing. The good news? Most people who act early get back to normal. No surgery. No scars. No long recovery. Just a splint, a few exercises, and a change in habits.Frequently Asked Questions
Can carpal tunnel syndrome go away on its own?
Rarely. Mild cases may improve with rest and splinting, but without addressing the root cause-like repetitive motion or poor wrist posture-the pressure returns. The nerve doesn’t heal itself once damaged. Waiting too long risks permanent numbness or muscle loss.
Is carpal tunnel syndrome caused by typing?
Not directly. Typing alone doesn’t cause it. But typing with your wrists bent, or for long hours without breaks, increases pressure in the carpal tunnel. It’s the combination of posture, duration, and force that matters. People who type with neutral wrists and take breaks rarely develop CTS.
How long does it take to recover from carpal tunnel surgery?
Most people return to light work in 2-3 weeks. Full recovery takes 6-8 weeks. Manual labor jobs may require 10-12 weeks. Endoscopic surgery often speeds things up by 2-3 weeks compared to open release. Pillar pain-tenderness near the incision-is common but usually fades in 6-12 weeks.
Are wrist splints effective for carpal tunnel?
Yes, especially for mild to moderate cases. Wearing a splint at night keeps the wrist straight, reducing pressure on the median nerve. Studies show 60-70% of patients see significant improvement after 4-6 weeks of consistent use. It’s the most recommended first-line treatment by orthopedic guidelines.
Can carpal tunnel come back after surgery?
It’s uncommon. Surgery cuts the ligament pressing on the nerve, which usually relieves pressure permanently. Recurrence happens in fewer than 5% of cases, often due to scar tissue or new injury. If symptoms return years later, it’s more likely a new problem-like arthritis or a different nerve issue-not the original CTS coming back.



















Write a comment
Your email address will be restricted to us